

Aetna Health and Inspira Health Partners entered into value-based program agreement on January 1, 2022 for the Medicare Advantage population. The goal of this agreement is for IHP to improve the coordination, clinical performance and cost of care for its attributed members. Aetna will compensate IHP for improved performance. Please see program details below.
2026 Program
Coming Soon
The Physician Distribution Formula is developed by the Finance Committee of Inspira Health Partners and approved by the Board.
Components of the formula include:
- Eligible funds will be prorated to primary care practices based on attributed lives.
- Measure performance will condition the payments to the practices
- Key Performance Indicators (KPI) measures (includes quality and care management) condition 75% of the payment
- Citizenship measures condition 25% of the payment
- Treatment of Unearned Dollars
- Re-distributed to practices who achieved a 75% score within the KPI category and 100% score within the citizenship category using a proration based on attributed lives (weighted at 75%)
- Reinvested in clinical integration initiatives (weighted at 25%)
Citizenship Metrics:

KPI Metrics:
Coming Soon
Coming Soon
Coming Soon
2025 Program
Medicare Advantage (MA) has two main funding sources: CMS which is the larger of the two, and monthly plan premiums paid by enrollees. The amount the MA plan receives from CMS depends on the county where the beneficiary lives, demographics (age and gender), and expected cost of the beneficiary based on acuity (risk-adjustment factor).
Aetna’s MA program sets a target for the Medical Loss Ratio (MLR) that decreases incrementally over a three-year contract period. Risk scores have a significant impact on this model, which are driven by hierarchical condition category (HCC) coding.
- Targets are different for individual and group plans
- Targets are set based on overall market performance and expected future year trends.
The base allocation between Aetna and IHP is 77/33. IHP is eligible to receive up to 33% of gross savings.
Quality metrics are scored separately based on a quality outcomes grid consisting of the star composite score and the average percentage of members seen. Quality metric targets are set annually by CMS.
The Physician Distribution Formula is developed by the Finance Committee of Inspira Health Partners and approved by the Board.
Components of the formula include:
- Eligible funds will be prorated to primary care practices based on attributed lives.
- Measure performance will condition the payments to the practices
- Key Performance Indicators (KPI) measures (includes quality and care management) condition 75% of the payment
- Citizenship measures condition 25% of the payment
- Treatment of Unearned Dollars
- Re-distributed to practices who achieved a 75% score within the KPI category and 100% score within the citizenship category using a proration based on attributed lives (weighted at 75%)
- Reinvested in clinical integration initiatives (weighted at 25%)
- Quality goals align with the 5-star threshold as outlined.
Citizenship Metrics:
KPI Metrics:
Coming Soon
Coming Soon
Coming Soon
2024 Program
Medicare Advantage (MA) has two main funding sources: CMS which is the larger of the two, and monthly plan premiums paid by enrollees. The amount the MA plan receives from CMS depends on the county where the beneficiary lives, demographics (age and gender), and expected cost of the beneficiary based on acuity (risk-adjustment factor).
Aetna’s MA program sets a target for the Medical Loss Ratio (MLR) that decreases incrementally over a three-year contract period. Risk scores have a significant impact on this model, which are driven by hierarchical condition category (HCC) coding.
- Targets are different for individual and group plans
- Targets are set based on overall market performance and expected future year trends.
The base allocation between Aetna and IHP is 77/33. IHP is eligible to receive up to 33% of gross savings.
Quality metrics are scored separately based on a quality outcomes grid consisting of the star composite score and the average percentage of members seen. Quality metric targets are set annually by CMS.
The Physician Distribution Formula is developed by the Finance Committee of Inspira Health Partners and approved by the Board.
Components of the formula include:
- Eligible funds will be prorated to primary care practices based on attributed lives.
- Measure performance will condition the payments to the practices
- Key Performance Indicators (KPI) measures (includes quality and care management) condition 75% of the payment
- Citizenship measures condition 25% of the payment
- Treatment of Unearned Dollars
- Re-distributed to practices who achieved a 75% score within the KPI category and 100% score within the citizenship category using a proration based on attributed lives (weighted at 75%)
- Reinvested in clinical integration initiatives (weighted at 25%)
- Quality goals align with the 5-star threshold as outlined.
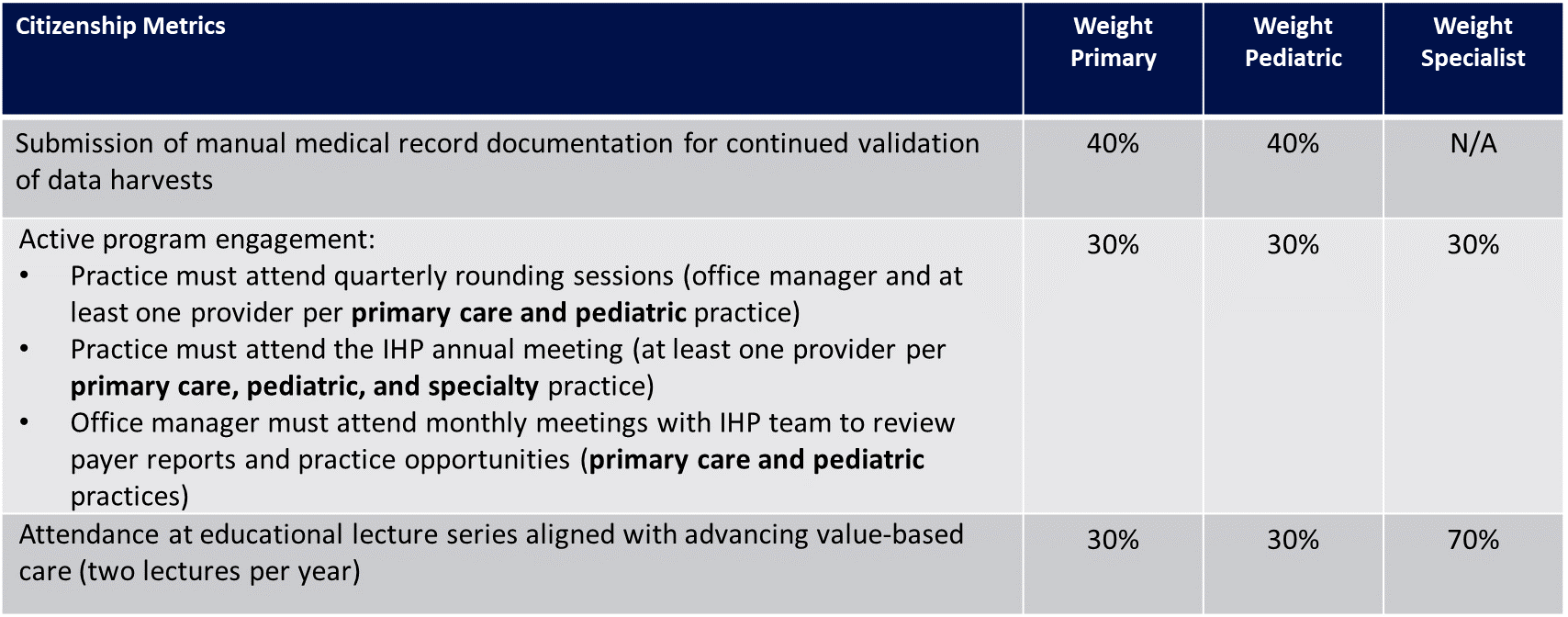
Citizenship Measures:
- Practice must submit EMR quality reports for continued validation of data harvests according to quarterly schedule (weighted at 15% of citizenship credit for primary care and 40% of citizenship credit for pediatric)
- Each provider must participate on the DoctusTech clinical documentation improvement program (weighted at 60% of citizenship credit for primary care)
- Active program engagement: (weighted at 15% of citizenship credit for primary care and 30% of citizenship credit for pediatric)
- Practice must attend quarterly rounding sessions (office manager and at least one provider per practice)
- Practice must attend the IHP annual meeting (at least one provider per practice)
- Office manager must attend monthly meetings with IHP team to review payer reports and practice opportunities
- Practice must attest to sending EMR direct messages for referrals and pass a quarterly audit (weighted at 10% of citizenship credit for primary care, 30% of citizenship credit for pediatric, and 100% of citizenship credit for specialists)
|
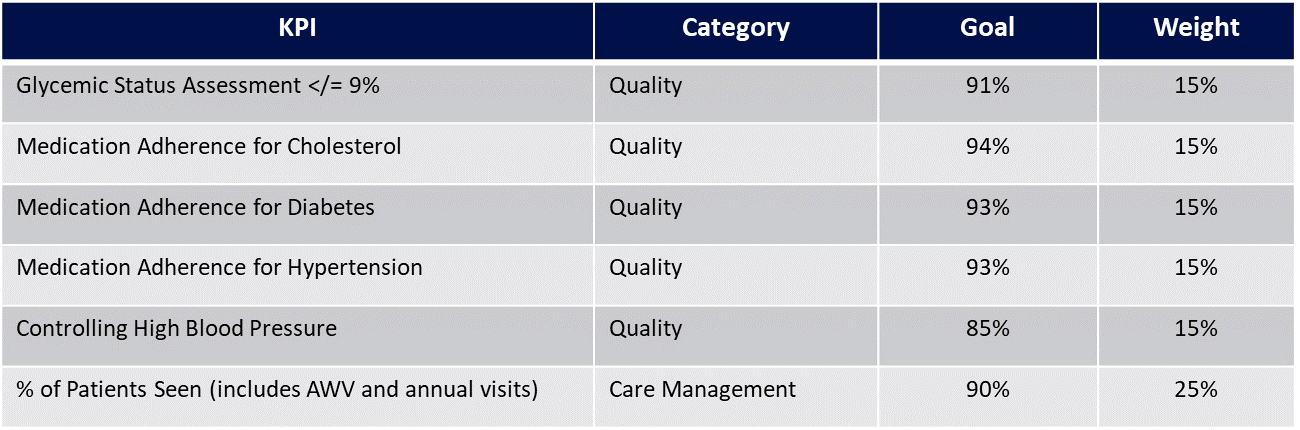
KPI |
Category |
Goal |
Weight |
|
Diabetic A1c Control < 8% |
Quality |
90% |
15% |
|
Medication Adherence for Cholesterol |
Quality |
93% |
20% |
|
Medication Adherence for Diabetes |
Quality |
90% |
20% |
|
Medication Adherence for Hypertension |
Quality |
93% |
20% |
|
% of Patients Seen (includes AWV and annual visits) |
Care Management |
90% |
25% |
Coming Soon
Aetna MA Program
2024 Citizenship Metric Performance
C = Compliant
NC = Non-Compliant
NA = Not Applicable
Coming Soon
2023 Program
Medicare Advantage (MA) has two main funding sources: CMS which is the larger of the two, and monthly plan premiums paid by enrollees. The amount the MA plan receives from CMS depends on the county where the beneficiary lives, demographics (age and gender), and expected cost of the beneficiary based on acuity (risk-adjustment factor).
Aetna’s MA program sets a target for the Medical Loss Ratio (MLR) that decreases incrementally over a three-year contract period. Risk scores have a significant impact on this model, which are driven by hierarchical condition category (HCC) coding.
- Targets are different for individual and group plans
- Targets are set based on overall market performance and expected future year trends.
The base allocation between Aetna and IHP is 77/33. IHP is eligible to receive up to 33% of gross savings.
Quality metrics are scored separately based on a quality outcomes grid consisting of the star composite score and the average percentage of members seen. Quality metric targets are set annually by CMS.
The Physician Distribution Formula is developed by the Finance Committee of Inspira Health Partners and approved by the Board.
Components of the formula include:
- Eligible funds will be prorated to primary care practices based on attributed lives.
- Measure performance will condition the payments to the practices
- Key Performance Indicators (KPI) measures (includes quality and care management) condition 75% of the payment
- Citizenship measures condition 25% of the payment
- Treatment of Unearned Dollars
- Re-distributed to practices who achieved a 75% score within the KPI category and 100% score within the citizenship category using a proration based on attributed lives (weighted at 75%)
- Reinvested in clinical integration initiatives (weighted at 25%)
- Quality goals align with the 5 star threshold as outlined.
- Citizenship Measures:
- Practice must submit EMR quality reports for continued validation of data harvests according to quarterly schedule (weighted at 15% of citizenship credit)
- Each provider must participate on the DoctusTech clinical documentation improvement program (weighted at 60% of citizenship credit)
- Active program engagement: (weighted at 15% of citizenship credit)
- Practice must attend quarterly rounding sessions (office manager and at least one provider per practice)
- Practice must attend the IHP annual meeting (at least one provider per practice)
- Practice must attest to sending EMR direct messages for referrals and pass a quarterly audit (weighted at 10% of citizenship credit)
| Key Performance Indicator | Category | Goal | Weight |
| Breast Cancer Screening | Quality | 75% | 10% |
| Colorectal Cancer Screening | Quality | 73% | 10% |
| Diabetic A1c Control <8% | Quality | 85% | 13.75% |
| Medication Adherence for Cholesterol | Quality | 94% | 13.75% |
| Medication Adherence for Diabetes | Quality | 94% | 13.75% |
| Medication Adherence for Hypertension | Quality | 93% | 13.75% |
| % of Patients Seen (includes AWV and annual visits) | Care Management | 90% | 25% |
| Annual PCV OV% | 96.9% |
| 2x Chronic OV% | 92.9% |
| OV AVG % | 95% |
Aetna MA Program
2023 Citizenship Metric Performance
C = Compliant
NC = Non-Compliant
NA = Not Applicable
Utilization data includes claims incurred from January through December 2023, paid through March 2024.
IHP’s MLR was 90.0%, higher than the target MCF of 87.5%, resulting in no savings.
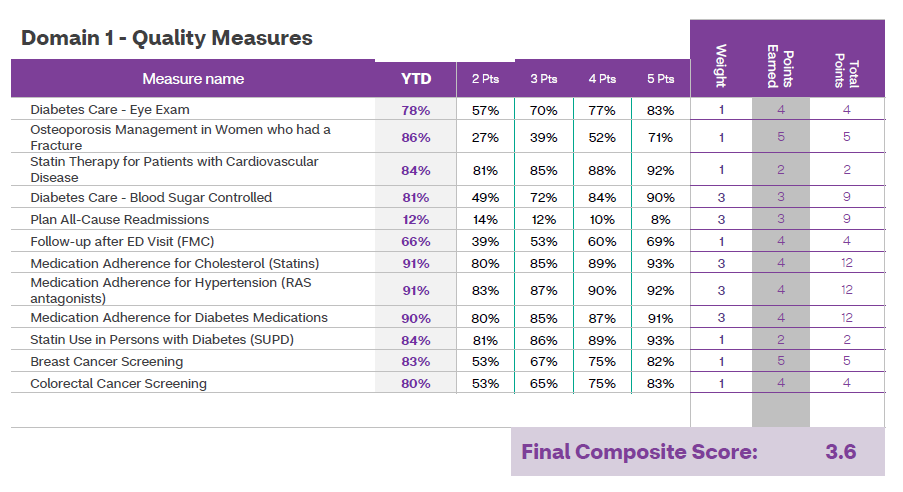
The Aetna MA program also includes 12 quality metrics that are rewarded separately from the MCF calculation. IHP scored 3.6 Stars on the quality portion and an average office visit score of 95%, resulting in a quality payment from Aetna. Please see the Quality Performance section for additional details.
Coming Soon
2022 Program
Medicare Advantage (MA) has two main funding sources: CMS which is the larger of the two, and monthly plan premiums paid by enrollees. The amount the MA plan receives from CMS depends on the county where the beneficiary lives, demographics (age and gender), and expected cost of the beneficiary based on acuity (risk-adjustment factor).
Aetna’s MA program sets a target for the Medical Loss Ratio (MLR) that decreases incrementally over a three-year contract period. Risk scores have a significant impact on this model, which are driven by hierarchical condition category (HCC) coding.
- Targets are different for individual and group plans
- Targets are set based on overall market performance and expected future year trends.
The base allocation between Aetna and IHP is 77/33. IHP is eligible to receive up to 33% of gross savings.
Quality metrics are scored separately based on a quality outcomes grid consisting of the star composite score and the average percentage of members seen. Quality metric targets are set annually by CMS.
Since the Aetna MA program was launched late in 2022, the IHP Board approved a distribution formula that combines reinvesting a portion of any savings earned towards clinical integration activities and distributing the remaining savings to practices based on a proration of attributed lives. The percentage to be reinvested will be determined using a tiered approach based on the overall savings amount.
|
Savings Amount |
% Reinvested in Initiatives |
% Distributed to Practices |
|
< $50k |
100% |
0% |
|
Between $50k and $100k |
40% |
60% |
|
> $100k |
20% |
80% |

Utilization data includes claims incurred from January through December 2022, paid through March 2023.
IHP’s MLR was 92.8%, higher than the target MCF of 88.4%, resulting in no savings.
The Aetna MA program also includes 14 quality metrics that are rewarded separately from the MCF calculation. IHP scored 4.0 Stars on the quality portion, resulting in a quality payment from Aetna. Please see the Quality Performance section for additional details.